Demystifying Creatine: Unpacking the Kidney Damage Myth
Welcome to our latest supplement-focused blog post. Today, we shift gears from introducing new supplements to dispelling the myths surrounding the 'DANGERS OF CREATINE!'
If you recall our recent blog on creatine, we detailed the numerous benefits of creatine monohydrate supplementation. While our overall health hinges mostly on our lifestyle choices, including diet and physical activity, supplements like creatine monohydrate can offer added advantages, particularly for those pursuing strength gains and cognitive health.
To get a comprehensive understanding of these benefits, revisit our earlier blog here.
If you’re not interested in checking that blog out, below is the International Society of Sports Nutrition's Position Statement on creatine.
Creatine monohydrate supplementation is not only safe, but has been reported to have a number of therapeutic benefits in healthy and diseased populations ranging from infants to the elderly. There is no compelling scientific evidence that the short- or long-term use of creatine monohydrate (up to 30 g/day for 5 years) has any detrimental effects on otherwise healthy individuals or among clinical populations who may benefit from creatine supplementation.
If proper precautions and supervision are provided, creatine monohydrate supplementation in children and adolescent athletes is acceptable and may provide a nutritional alternative with a favorable safety profile to potentially dangerous anabolic androgenic drugs. However, we recommend that creatine supplementation only be considered for use by younger athletes who: a.) are involved in serious/ competitive supervised training; b.) are consuming a well-balanced and performance enhancing diet; c.) are knowledgeable about appropriate use of creatine; and d.) do not exceed recommended dosages.
Label advisories on creatine products that caution against usage by those under 18 years old, while perhaps intended to insulate their manufacturers from legal liability, are likely unnecessary given the science supporting creatine’s safety, including in children and adolescents.
At present, creatine monohydrate is the most extensively studied and clinically effective form of creatine for use in nutritional supplements in terms of muscle uptake and ability to increase high- intensity exercise capacity.
The addition of carbohydrate or carbohydrate and protein to a creatine supplement appears to increase muscular uptake of creatine, although the effect on performance measures may not be greater than using creatine monohydrate alone.
The quickest method of increasing muscle creatine stores may be to consume ~0.3 g/kg/day of creatine monohydrate for 5–7-days followed by 3–5 g/day thereafter to maintain elevated stores. Initially, ingesting smaller amounts of creatine monohydrate (e.g., 3–5 g/day) will increase muscle creatine stores over a 3–4 week period, however, the initial performance effects of this method of supplementation are less supported.
Clinical populations have been supplemented with high levels of creatine monohydrate (0.3 – 0.8 g/kg/ day equivalent to 21–56 g/day for a 70 kg individual) for years with no clinically significant or serious adverse events.
Further research is warranted to examine the potential medical benefits of creatine monohydrate and precursors like guanidinoacetic acid on sport, health and medicine.

In case the ISS's position statement doesn't quite resonate with you, the IOC's Consensus Statement from their research article, "IOC consensus statement: dietary supplements and the high-performance athlete," provides a comprehensive review as well. You can see a synopsis of their statement in the 2 pictures on the right. The consensus statements from these organizations are based on numerous long-term studies on creatine monohydrate supplementation.

Why Does Stigma Persist?
Despite the prevailing evidence supporting the safety of creatine, one myth continues to persist - 'creatine is bad for your kidneys.'
Why does this misconception endure?
It starts with a study published in 1998, one of the first case reports that drew the conclusion, “There is strong circumstantial evidence that creatine was responsible for the deterioration in renal function in this case.” Since that time this study has continue to be cited throughout the literature as foundational piece of the argument, “Creatine is bad for your kidneys.”
However, when looking at this case report there a few key points that cannot be dismissed. First the 25 year old individual who had decreased kidney function, who in the authors opinion was due to creatine supplementation already had kidney dysfunction before starting to supplement with creatine.
In fact the individual before starting creatine supplementation had, Focal Segmental Glomerulosclerosis (FSGS) and due to that had re-occurent nephrotic syndrome. FSGS is a disease in which scar tissue develops on the parts of the kidneys that filter waste from the blood (glomeruli). FSGS can be caused by a variety of conditions, though sometimes it occurs without a known cause. Due to this individual’s FSGS he developed nephrotic syndrome that would be relieved by taking the immunosuppressant cyclosporin.
So the individual in this case had abnormal functioning kidneys that resulted in further impairment of the kidneys due to nephrotic syndrome and he was treated with a cyclosporin which is known to be toxic to the kidneys over long periods of times and at high doses.
This was occurring for 5 years prior to any supplementation with creatine. This individual then started supplementing with creatine and returned to the medical office for routine lab work. He was in good health, had no signs of kidney dysfunction or nephrotic syndrome. However, upon doing test in the lab his kidneys showed a decreased ability to filter waste products from his blood, the only thing that changed during this time according to the individual was starting creatine supplementation. Upon finding these values of kidney functions being negatively impacted by creatine he was advised to quit taking creatine and within a month his labs returned to normal.
An individual with mild kidney disease that would progress to severe kidney disease without continued treatment had altered kidney function due to creatine supplementation.
Based off of this I think it is scientifically unsound to draw broad conclusions about creatine safety based on a single case report, particularly when the subject had a pre-existing kidney disease and was also taking a medication known to be toxic to the kidneys (nephrotoxic). Yet, this study is seen throughout the literature as one of the foundational arguments that creatine is bad for your kidneys.
The overwhelming body of scientific evidence indicates that creatine supplementation is safe for healthy individuals, with numerous studies finding no significant side effects associated with its long-term use at standard doses. These research studies provide a more reliable basis for conclusions about creatine's safety.
Transient increases in creatinine levels, which can occur due to increased muscle activity or creatine supplementation, do not necessarily signal a decrease in kidney function. If anything, this case study serves as a reminder for individuals with kidney disease to consult their doctors before starting creatine supplementation, not only because of possible risks but also potential benefits they might miss out on by avoiding creatine.
Another one.
Another study that is often cited in the literature as a warning about creatine is another case report. This one from 2003. We aren’t going to dive as deep as we did into the last one because it’s pretty cut and dry. A 22 year old male was taking Dianabol an illegal anabolic steroid known to cause kidney problems and was also supplementing with 200 grams of creatine a day, 10 times higher than the upper recommended limit of daily creatine supplementation. The individual developed kidney issues.
This case report suggests a link between anabolic steroid use, high-dose creatine supplementation, and renal damage. However, drawing the conclusion that creatine alone is harmful to the kidneys based on one individual who who took 10 times the upper limit of the recommended dose while on anabolic steroids is problematic for several reasons.
Firstly, the individual in question was using methandienone, an anabolic steroid. Anabolic steroids are well-known for their potential to cause kidney damage. They can lead to high blood pressure, a significant risk factor for kidney disease, and directly cause damage to the kidneys over time. Therefore, it is highly likely that the anabolic steroid use played a significant role in this individual's kidney damage.
Secondly, the creatine dose this person was taking was extremely high. The report states he was consuming 200 grams of creatine daily, which is far beyond the typical recommended dose of 3-5 grams per day after a loading phase. Such an extraordinarily high dose could potentially stress the kidneys, but this is not reflective of standard, responsible use of creatine.
Lastly, this is a single case report, which is a form of anecdotal evidence. While case reports can be valuable for generating hypotheses or pointing towards potential rare side effects of a substance, they are not designed to establish cause and effect relationships. As such, conclusions drawn from a single case report should be viewed with caution, as they may not apply to the general population.
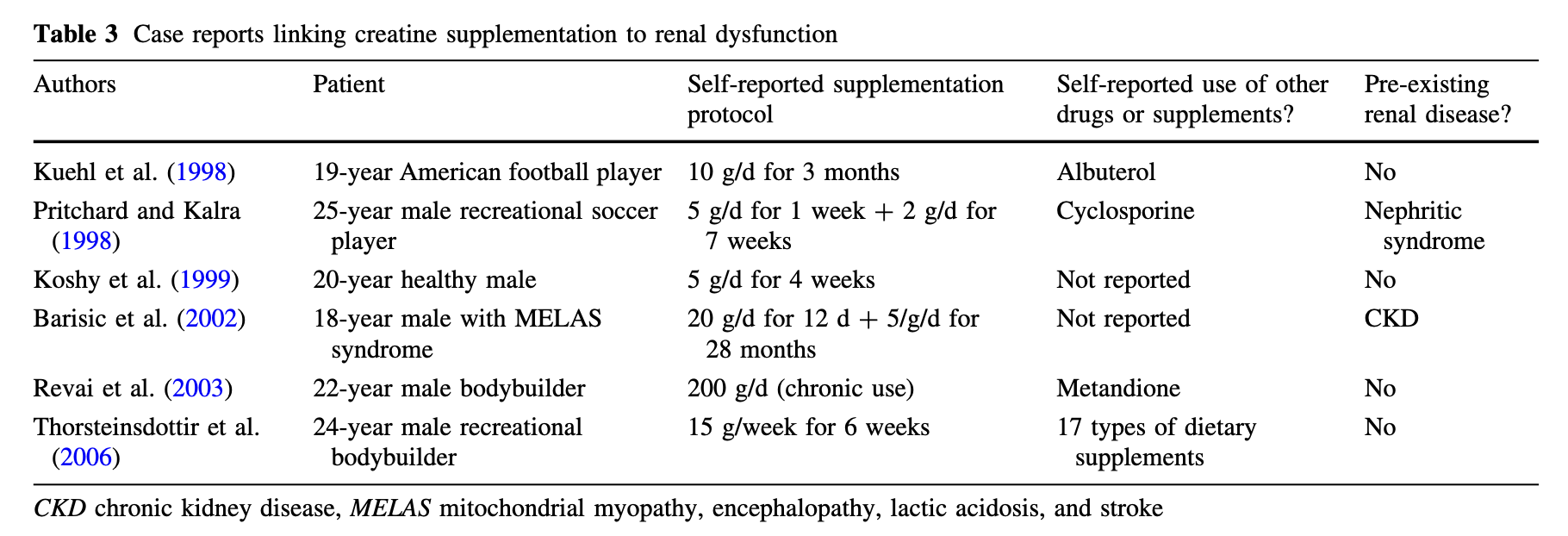
There have been a few other case studies that continually show up in the literature and the author’s, Gualano B, Roschel H, Lancha AH Jr, Brightbill CE, and Rawson ES provide us a nice overview of these in their research article, In sickness and in health: the widespread application of creatine supplementation, you can see this overview to the right.
We could continue to delve into the numerous case reports scattered throughout scientific literature over time, each purporting that creatine causes kidney dysfunction, but these reports usually follow a similar pattern:
There is more than one possible cause of decreased kidney function, but the authors conclude that creatine is the differential factor.
The case reports are often based on a single individual ('N=1') with no comprehensive studies on large groups having negative effects from creatine supplementation.
The warnings about creatine negatively affecting the kidneys continue to cite the same few case reports repetitively, with scarce additions of new reports with similar findings.
In reality, creatine monohydrate is safe. In some exceedingly rare instances where kidney function is greatly limited, the kidneys are diseased, or other extenuating circumstances are present, creatine supplementation can impose additional stress on the kidneys and is thus not recommended. Nevertheless, these circumstances should not excuse the scientific and medical communities from making blanket statements like 'Creatine is bad for your kidneys.' Such statements are not only inaccurate but harmful.
They instigate fear around creatine supplementation without concrete, broad-scale scientific evidence, potentially deterring individuals from reaping its proven benefits. As with any supplement, it's essential to use creatine responsibly, adhering to recommended dosages, and for individuals with any pre-existing conditions to consult their healthcare providers before starting supplementation.
The primary takeaway here is: blanket generalizations are dangerous and often misleading. Just as one wouldn't declare all fruits harmful because some people are allergic to strawberries, it's irrational to label creatine as harmful based on a handful of cases, especially when the majority of scientific evidence supports its safety and efficacy.
As always I hope you enjoyed this blog and if you have any questions feel free to reach out to me at drcoffman@optimizecolumbus.com.
References
Antonio J, Candow DG, Forbes SC, Gualano B, Jagim AR, Kreider RB, Rawson ES, Smith-Ryan AE, VanDusseldorp TA, Willoughby DS, Ziegenfuss TN. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J Int Soc Sports Nutr. 2021 Feb 8;18(1):13. doi: 10.1186/s12970-021-00412-w. PMID: 33557850; PMCID: PMC7871530.
Barisic N, Bernert G, Ipsiroglu O, Stromberger C, Müller T, Gruber S, Prayer D, Moser E, Bittner RE, Stöckler-Ipsiroglu S. Effects of oral creatine supplementation in a patient with MELAS phenotype and associated nephropathy. Neuropediatrics. 2002 Jun;33(3):157-61. doi: 10.1055/s-2002-33679. PMID: 12200746.
Gualano B, Roschel H, Lancha AH Jr, Brightbill CE, Rawson ES. In sickness and in health: the widespread application of creatine supplementation. Amino Acids. 2012 Aug;43(2):519-29. doi: 10.1007/s00726-011-1132-7. Epub 2011 Nov 19. PMID: 22101980.
Révai T, Sápi Z, Benedek S, Kovács A, Kaszás I, Virányi M, Winkler G. Súlyos fokú nephrosis szindróma kialakulása anabolikus szteroidot és kreatint tartósan szedó fiatal férfiban [Severe nephrotic syndrome in a young man taking anabolic steroid and creatine long term]. Orv Hetil. 2003 Dec 7;144(49):2425-7. Hungarian. PMID: 14725210